The early signs of an orthopedic condition may be detected in children at birth or over the course of their early years up until their teenage years. Other than the child’s pediatrician, you – the parent – also play a significant role in detecting the condition early on.
The best time to consult your doctor is whenever you, as the parent, feel that something is not right with your baby or child in terms of posture, movement or any other signs. The earlier a bone deformity is diagnosed, the more successful the treatment will be.
The age at which symptoms present themselves varies from child to child. Some bone deformities are evident at birth, such as clubfoot, while others may present themselves between 10 and 18 years of age, such as scoliosis. To learn more about various orthopedic conditions that may affect children, you may look here.
During your doctor’s visit, the doctor will carefully examine your child and explain to you in detail the child’s diagnosis (if any). Additionally, they will explain the best treatment option that is appropriate for the child. For more information on surgical and non-surgical treatment options, you may look here.
The doctor may also request for additional X-rays, blood and/or nerve tests to assist with their diagnosis. It is important that you feel comfortable asking your doctor any questions about your child’s diagnosis and treatment. The better informed you are, the more comfortable you and your child will be during the course of treatment. You may look here for more guidance on finding the right surgeon.
The younger a child is, the more flexible their bodies are, making early detection a challenge sometimes. However, a parent’s intuition is a great indicator and if you feel something is “just not right,“ then you should book an appointment with your pediatrician and get your child examined. During your child’s routine checkups, the pediatrician does a series of tests by moving the child’s limbs in a certain manner to look for characteristic signs of some orthopedic conditions. However, as a parent, you may also want to look out for certain indicators as well.
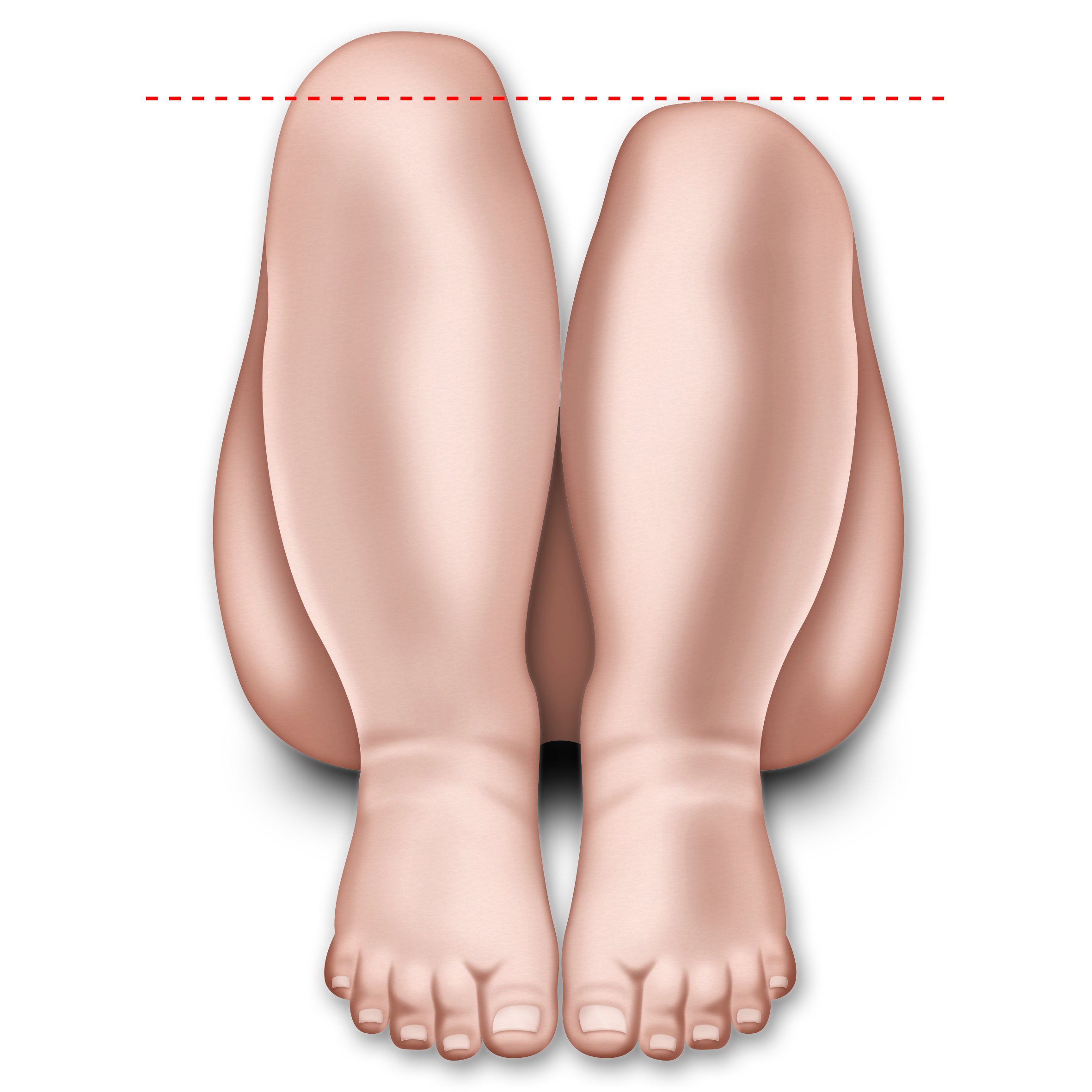
Signs to look out for include (but are not limited to):
- Legs of different lengths, as shown here:
- Uneven skin folds on the thigh
- Restricted movement in one leg when you change their nappy or diaper
- One leg dragging behind the other when they crawl
- Less mobility or flexibility on one side
- Limping, toe walking, or a waddling gait
- Short stature
- Breathing problems
- Hearing issues
- Brittle teeth
- Bowed legs
- Blue sclera (the part of the eye that is usually white)
- Curved spine
- Child has changed posture over time; especially while playing sports, running style has changed and doesn’t “look normal”
- Child complains of intermittent pain in the groin, hip, knee and/or thigh
- Inability to walk or bear weight on one leg
- Outward turning (external rotation) of one leg
- Turning in of the feet (intoeing)
If any of the above symptoms are presenting in your child, it is best to book an appointment at the earliest opportunity with your child’s pediatrician who, upon examination, may refer you to an orthopedic doctor for further tests.
With the increasing prevalence of diabetes in the world, patients need to be aware of early detection signs in the feet for diabetes related orthopedic complications.
0.3% to 7.5% of diabetic patients may develop a Charcot neuroarthropathy. Diabetic neuropathy (i.e. nerve damage) and peripheral vascular disease (i.e. poor circulation) are two of the main foot problems that occur, and both can have serious complications. If left untreated, this condition leads to deformity, ulcers and infection and – in the worst case – to amputation. Worldwide, 85 percent of leg amputations are a result of a diabetic foot ulcer. Up to 80% of diabetic patients are more likely to die within 5 years of having a limb amputation. However, 4 out of 5 amputations can be prevented. Timely diagnosis facilitates treatment and decreases long-term disability. Therefore, it is essential for diabetic patients to be aware of the early detection signs for diabetes related foot problems.
Nerve damage and poor circulation in the feet may lead to numbness or lack of sensation. This means that if a patient with diabetic foot develops an ulcer or infection in their foot, they would not be able to recognize it as the sensation of pain or irritation is largely reduced or completely absent. They would not realize that their feet require medical attention. This unintentional ignorance may lead to a buildup of gangrene, which, if left untreated, leads to a possibility of foot amputation as a worst case scenario.
Complications of diabetic foot problems include:
- Foot ulcers or wounds that do not heal
- Infections, including skin infections, bone infections, and abscesses
- Gangrene, when an infection causes tissue death
- Foot deformity
- Charcot foot and ankle, which alters the shape of the feet as bones in the foot and toe shift or break
Foot and ankle surgeons are qualified to detect the early stages of diseases that exhibit warning signs in the lower extremities, such as diabetes, arthritis and cardiovascular disease, and they manage foot conditions that may pose an ongoing threat to a patient’s overall health.
Your surgeon should treat any complications arising from diabetes, help your wounds heal and avoid amputation; amputation is a last resort when no other treatment option is working.
Your role is key in preventing and reducing complications by:
- Having a preventive foot evaluation every year
- Examining foot skin and nails daily: check for cuts, blisters, redness, swelling or nail problems
- Keeping your feet clean by washing them daily using lukewarm (not hot) water
- Moisturizing your feet but not between your toes as fungal infections are most common here
- Having regular expert podiatric care: do not treat/cut/trim your corns or calluses yourself
- Ensuring that your socks are clean and dry. Change them throughout the day if you live in a humid region. Some socks are available specifically for diabetic patients to help avoid buildup of moisture. You may ask your doctor or local pharmacy about this
- Choosing appropriate footwear
- Always wear waterproof footwear in wet weather. It is essential to keep your feet warm and dry and not let your feet get wet in snow or rain. You may use an antiperspirant on the soles of your feet to absorb extra sweat
- Do not walk barefoot, as you may step on something and injure yourself
- Replacing orthotic shoes every year: they should fit perfectly
- Reporting absence of pain when it should be felt (e.g. touching hot water)
- Stopping or reducing smoking
- Reducing alcohol
If you notice any of the following changes, you should seek immediate medical attention:
- Warm, swollen, red foot and/or ankle
- Continuous unpleasant odor from the foot
- Higher temperature of 2°C or 4°F of one foot compared with the contralateral one
- Interdigital maceration
- Skin lesions, ulcers and open wounds
- Hypertrophic calluses or corns
- Discolored, ingrown nails
- Crepitant cellulitis
- Fungal infection on the feet
- Bone deformities
- Loss of foot sensitivity
- Limited range of joints motion
- Absence of Achilles tendon reflex
- Vascular compromise, with sudden absence of dorsalis pedis and posterior tibial pulses
- Peripheral arterial disease
- Diabetic gangrene and necrosis
- Previous amputation
Non-surgical: the first attempt would be to treat a diabetic foot without using surgery. This is possible if the condition is caught early on. Some methods include:
- Continuous cleaning and dressing of the wound/infection site on the feet
- Immobilization devices, such as a cast boot or total contact cast, may be provided to the patient
- In some cases, self-amputation occurs, which is when the toes fall off due to lack of blood flow
Surgical: when non-surgical treatment does not successfully heal diabetic foot problems, the doctor might consider surgery. Many new surgical techniques are available to avoid amputation, such as joint reconstruction and wound healing technologies. Regular checkups with your doctor may help catch problems at an early stage, which is crucial to get effective treatment. A proactive approach by the patient is crucial; visit your doctor as soon as a symptom is observed. Surgical treatment options include:
- The removal of decaying or dead tissue
- Surgical stabilization of Charcot foot and ankle. In presence of severe deformities – that cannot be treated in a brace – osteotomy, fixation and temporary off-loading can help to correct deformities
- An arterial bypass for peripheral vascular disease, which assists blood flow to the area
- Endovascular surgery with placement of stents, which uses small devices to keep blood vessels open
Even with preventive care and prompt treatment of infection and complications, there are instances when amputation is necessary to remove infected tissue, save a limb or even save a life. Amputation, ranging from single toes or sections of foot to amputation of the leg below or even above the knee, is the worst case scenario and requires the surgeon to remove the infected portion of the leg to avoid further spread of infection.
For more information regarding diabetes and related foot care you may look here and here.